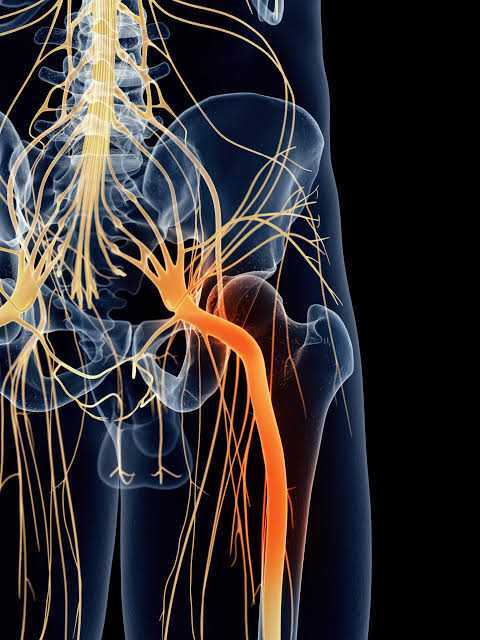
Lateral hip pain
Lateral hip pain is very common and debilitating source of pain. There are multiple pathologies associated with anatomical structures of the lateral hip including:
• Gluteal tendinopathy
• Gluteal bursitis
• Gluteal tears
• External snapping hip syndrome
• Proximal ITB syndrome
Pain in this region has been termed Greater Trochanteric Pain Syndrome (GTPS) which is an umbrella term. GTPS signs and symptoms usually consist of
• Px directly over the GT
• Referral into lateral thigh and lower leg
• Px with walking hills and stairs
• Px with sitting
• Px with laying on side
• Hopping, running or jumping


Traditionally treatment for GTPS involved ice and stretching…

But what’s in a name?
• Syndrome is a cluster of symptoms
• The name “syndrome” may have negative effects on patient’s thoughts, beliefs and engagement with treatment
• Leaves uncertainty in treatment direction
Long et al (2013) performed ultrasound on 877 patients with GTPS and 80% did not have bursitis on ultrasound.
Should we really be using the term bursitis? This term suggests that there is an inflammatory component and this is often interpreted as rest, Ice and take NSAID however this may be unhelpful in recovery. Connell et al (2003) found that only 8 of 75 hip had fluid pooling in the greater trochanteric bursa in subjects with gluteal tendinopathy.
Ruta et al (2015) fount that Bursitis as the only abnormal finding on ultrasound occurred in 4% of examination whereas tendinopathy of Gluteus Medius and minimus was found in 50% of subjects.
Bursitis certainly exists and may be a contributor to the pain. Fearon et al (2014) Showed significantly increased levels of substance P in the Bursa but not the tendon in subjects with GTPS. This nociceptive role could explain why bursectomy is sometimes helpful in persistent GTPS. However, bursitis is often secondary to gluteal tendinopathy and therefore should not be labelled as nor treated as the primary cause. Furthermore, the inflammatory component often suggests a more passive role in rehabilitation and is often considered for corticosteroid injection. Dean et al (2014) demonstrated that CSI has significant negative long-term effects on tendon tissue and cells. This could be a further contributor to the chronicity of lateral hip pain.
Gluteal tendinopathy is the most prevalent lower limb tendinopathy.
What are the risk factors for gluteal tendinopathy?
• Increase Age
• Gender
• Genetics
• Smoking
• Obesity & metabolic factors
• Diabetes
• Medications
• Steroids
• Fluoroquinolones
• Statins
• History of injury
• Change in activity
• Overload
• Changes in exercise volume, frequency, or intensity
• Inappropriate rest
• Underload
• High cholesterol
• Smoking
• Muscle strength
• Rheumatological conditions
Gluteal tendinopathy is most prevalent in peri and post-menopausal women. Estrogen plays an important role in collagen synthesis; therefore estrogen deficiency can have negative effects on tendon health. The reduction in collagen synthesis leads to matrix degeneration, reduced fiber diameter reduced collagen density and reduced ability to withstand tensile load.
Gluteal tendons are vulnerable to compression as they attach to the greater trochanter. With the hard bony surface of the greater trochanter underneath the tendons and the thick fibrous band of the ITB laying over the top of the tendon this makes the gluteal tendons very vulnerable to compression. Compression can cause changes to the collagen matrix which can impair the tendon’s ability to withstand tensile load. Here are some factors that may increase compression:
• Prolonged sitting (particularly with legs crossed or knees kissing)
• Laying on side
• Hanging on one hip
• SL standing, incline or hill walking / hill running
• Rapid change in activity
• Running, jumping, landing







Removing these provocative factors are key to the successful management of GTPS in combination with progressive loading.
Bodine Ledden